A- Surgical Treatments of Obesity
1- Tube Stomach Surgery
2- Gastric Balloon
3- Mini Gastric Bypass Operation
4- RNY Gastric Bypass Operation
5- Revisional Bariatric Surgery
A- Surgical Treatments of Obesity
1- Tube Stomach Surgery
2- Gastric Balloon
3- Mini Gastric Bypass Operation
4- RNY Gastric Bypass Operation
5- Revisional Bariatric Surgery
OBESITY SURGICAL PROCEDURES
GASTRIC BOTOX:
As it has been observed to have limited long-term benefits, Polidia Health does not recommend or perform this operation for our patients.
RNY GASTRIC BYPASS SURGERY
General Characteristics
MECHANISM OF ACTION
Since the excessive or rapid consumption of high-calorie foods (especially those containing carbohydrates) can cause discomfort for patients, they tend to adopt healthier eating habits. (Patients often exhibit a tendency to avoid sweet and fatty foods).
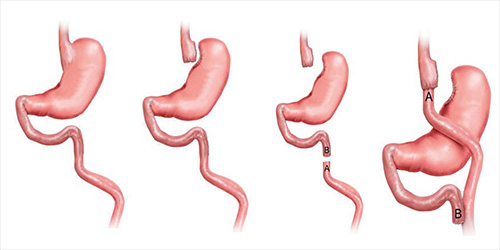
In the first image, the esophagus, stomach, and the beginning of the small intestine are shown. In the RNY Gastric Bypass surgery, the upper part of the stomach is divided into a small and a large portion using staples, allowing the patient to eat smaller portions (restriction effect). The small intestine is divided (A) and prepared for connection to the reduced stomach. The small intestine (A) is pulled up and connected to the reduced stomach using a circular stapling method. At a point further down from the newly created small stomach-intestine connection, the remaining intestine (B) from the original stomach is reconnected to the main tract. This allows the fluids and enzymes produced by the remaining stomach (B) to continue their normal path together with the ingested food, ensuring that essential vitamins are still absorbed by the body without any deficiencies.
One of the significant advantages of this surgery is that the ingested food and the fluids (enzymes, bile, and pancreatic secretions) produced by the remaining (non-food receiving) stomach join together at a later point. As a result, the absorption of fat and sugar, i.e., calorie absorption, is reduced. (malabsorptive effect)
Moreover, the smaller passage from the reduced stomach to the intestine slows down the stomach emptying, creating a longer-lasting feeling of fullness in the patients.
Sleeve Gastrectomy (Gastric Sleeve)
Sleeve Gastrectomy | General Characteristics
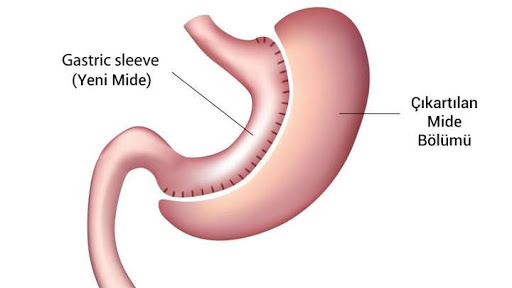
In Sleeve Gastrectomy, approximately 80% of the stomach is divided and removed using staples, leaving behind a long tube-like structure. This is why the procedure is called “Sleeve” Gastrectomy in English and “Tüp Mide” (Tube Stomach) in Turkish. A person who has undergone Sleeve Gastrectomy may consume less food compared to normal, but since there is no decrease in the absorption of consumed food, the calories from the ingested food are fully absorbed by the body. As a significant portion of the stomach is removed during Sleeve Gastrectomy, this type of operation is not reversible.
What is Sleeve Gastrectomy, and How is it Performed? Sleeve Gastrectomy is usually performed laparoscopically, meaning it is done through small incisions. Five small incisions are made to enter the abdominal cavity. Sleeve Gastrectomy is purely a restrictive operation and does not have any malabsorptive effect.
In the image, the normal state of the stomach is shown.
The ingested food accumulates in the stomach and, after passing into the small intestine, the calories from this food are fully absorbed by the body.
In Sleeve Gastrectomy, approximately 80% of the stomach is divided and removed using staples. The remaining part takes on the shape of a tube, which is why this operation is called Sleeve Gastrectomy or “Tüp Mide” in Turkish.
As a result of Sleeve Gastrectomy, the amount of food consumed decreases due to the reduced stomach capacity, but calorie absorption remains the same. This is one of the disadvantages of this operation. In other words, someone who consumes small amounts of high-calorie foods still absorbs all the calories. This can lead to an increased rate of weight regain after Sleeve Gastrectomy. Another disadvantage is the destruction of approximately 80% of the stomach, making it impossible to return to its original state
Mini Gastric Bypass Surgery

General Characteristics
The difference from RNY Gastric Bypass is that in Mini Gastric Bypass, the intestine is connected to the stomach without dividing it. As a result, in Mini Gastric Bypass surgery, one less connection is made compared to RNY Gastric Bypass.
The reduction in absorption is achieved by bypassing a longer section of the intestine in Mini Gastric Bypass surgery compared to RNY Gastric Bypass.
Due to the remaining stomach’s location as the passage for fluids and subsequently bile, there is a possibility of bile reflux in Mini Gastric Bypass surgery.
Throughout my professional career, I always maintained a reserved attitude towards gastric balloon applications, one of the non-surgical weight loss methods. The main reason for this was the observed lack of desired weight loss in individuals who underwent gastric balloon procedures, and in some cases, even gaining extra weight despite having the balloon in their stomachs.
It was quite puzzling that individuals with a small fluid-filled balloon in their stomachs, roughly the size of a small water bottle, were unable to lose weight, and some even gained weight. With this concern in mind, I embarked on an extensive research. Over time, I discussed the topic with a close colleague who had achieved successful results with balloon applications on the international stage. The logical ideas he advocated also changed my perspective on gastric balloons. Individuals who had gastric balloons inserted were achieving better weight loss rates, and they did not regain weight after the balloon was removed. The key factor he emphasized for permanent weight loss was the dietary approach. Thanks to him, I witnessed many misconceptions about nutrition that were considered true to be refuted. I say I witnessed because, thanks to this sensible method, we began to observe surprising rates of weight loss in our patients after gastric balloon applications.
Based on these observations, I can now confidently say that if you also want to lose weight permanently without surgery, you can contact us to get more detailed information.
Now, let’s discuss which type of gastric balloon should be preferred: the classic type or the swallowable type.
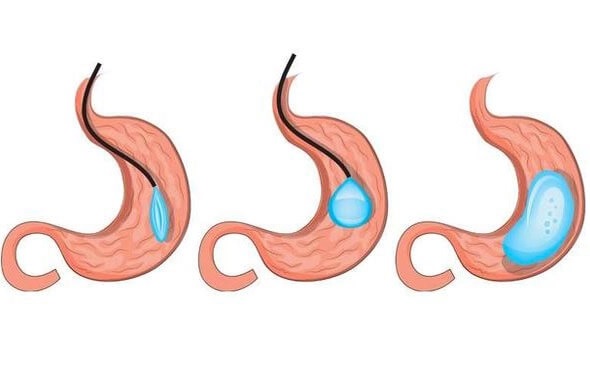
In this method, the balloon is placed in the person’s stomach through endoscopy. Before the procedure, the person is lightly sedated. Then, a camera called an endoscope, in the shape of a hose, is inserted into the esophagus and stomach to view the interior. If there are no obstacles to placing the balloon, it is inserted into the stomach and inflated with a special fluid of half-liter. Approximately six months later, the balloon is removed from the stomach using endoscopy.
ADVANTAGES DISADVANTAGES • The inside of the stomach is viewed with a camera before placing the balloon
Requires mild anesthesia Effectiveness lasts for 6 months Removed with endoscopy after 6 months More economical
In this method, the balloon is relatively larger and is swallowed by the person with the help of water. Afterward, an abdominal X-ray or similar imaging is done to check if the balloon has descended into the stomach. If the balloon has reached the stomach, it is inflated with a special fluid using a catheter attached to the back of the capsule. Another imaging is taken to verify if the balloon is inflated or not. This type of gastric balloon naturally disintegrates and passes out through the intestines within approximately 4 months. However, the disintegrated balloon may cause intestinal blockages in some individuals, necessitating surgery.
ADVANTAGES DISADVANTAGES
Revisional obesity surgery involves changing the obesity surgery that was previously performed on a patient but yielded insufficient or unsuccessful results by applying other obesity surgery methods.
The duration of these operations depends on the previous surgery and usually takes 1-3 hours. The patient’s hospital stay is typically 3-4 nights.